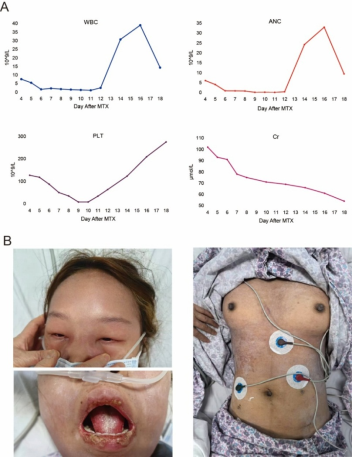
Low-dose methotrexate (LD‑MTX) is widely regarded as a safe and effective fertility‑preserving treatment for selected ectopic pregnancies; however, rare cases of severe, life‑threatening toxicity have been reported. We describe a previously healthy 24‑year‑old woman who developed fulminant systemic toxicity following a single intramuscular dose of 60 mg methotrexate administered for persistent tubal ectopic pregnancy after laparoscopic salpingostomy. Within 72 hours, she presented with progressive mucocutaneous manifestations, including diffuse rash, facial oedema and severe oral ulceration, followed by pancytopenia and acute kidney injury by day 4. Concomitant treatment with long‑acting benzathine penicillin G and subsequent pharmacogenetic testing revealing heterozygous MTHFR C677T and MTRR A66G variants were considered contributory risk factors. Prompt initiation of high‑dose intravenous leucovorin rescue, alkalinised hydration and granulocyte colony‑stimulating factor led to complete haematological recovery by day 14 and normalisation of renal function without the need for glucarpidase or extracorporeal clearance. A review of the literature identified fewer than a dozen similar cases, highlighting consistent early mucocutaneous warning signs and rapid progression to severe myelosuppression. This case underscores that even a single LD‑MTX dose can precipitate severe toxicity when renal clearance is impaired, interacting medications are present and folate‑pathway polymorphisms coexist, and emphasises the critical importance of early symptom recognition, close laboratory monitoring between days 4 and 7, and timely leucovorin rescue.
| Published in | Journal of Gynecology and Obstetrics (Volume 14, Issue 1) |
| DOI | 10.11648/j.jgo.20261401.13 |
| Page(s) | 30-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Methotrexate Toxicity, Ectopic Pregnancy, Pharmacogenetics, MTHFR, OAT3, Leucovorin Rescue
Date (Days after MTX) | WBC (10^9/L) | ANC (10^9/L) | Hb (g/L) | PLT (10^9/L) | CRP (mg/L) | Cr (μmol/L) | β- hCG | CMTX (μmol/L) |
|---|---|---|---|---|---|---|---|---|
2025/6/2 (D4) | 7.58 | 6.06 | 116 | 127 | 27.8 | 102 | 97.14 | |
2025/6/3 (D5) | 5.48 | 4.07 | 111 | 118 | 93 | |||
2025/6/4 (D6) | 1.64 | 0.89 | 100 | 87 | 91 | 47.12 | ||
2025/6/5 (D7) | 2.19 | 0.85 | 92 | 50 | 78 | 0.08 | ||
2025/6/6 (D8) | 1.78 | 0.78 | 84 | 35 | 75 | 0.09 | ||
2025/6/7 (D9) | 1.46 | 0.14 | 87 | 8 | ||||
2025/6/8 (D10) | 1.26 | 0.18 | 84 | 8 | 56.82 | 71 | ||
2025/6/9 (D11) | 1.05 | 0.1 | 76 | 34 | ||||
2025/6/10 (D12) | 2.5 | 0.39 | 80 | 63 | 69 | |||
2025/6/12 (D14) | 30.69 | 24.2 | 85 | 123 | 17.63 | 66 | ||
2025/6/14 (D16) | 39 | 32.97 | 85 | 209 | 8.93 | 61 | ||
2025/6/16 (D18) | 14.29 | 9.42 | 90 | 275 | 5.94 | 54 | 0.367 |
Drug | Gene | Test Locus | Evidence Level | Test Method | Test Result |
|---|---|---|---|---|---|
Folic Acid | MTHFR | C677T | 3 | Real-time fluorescent PCR | C/T (heterozygous) |
MTHFR | A1298C | 3 | Real-time fluorescent PCR | A/A (wild type) | |
MTRR | A66G | 3 | Real-time fluorescent PCR | A/G (heterozygous) |
Reference* | NO. | Age (yr) | Baseline renal function | Concomitant Medications | Folate supplementation | Symptom to onset interval | Major clinical findings | Interventions | Outcome |
|---|---|---|---|---|---|---|---|---|---|
Stavros [1 7] | 1 | 32 | Normal | Not reported | Yes | 5 days | High fever, pancytopenia | MTX withdrawal + high-dose leucovorin, G-CSF,supportive care | Recovery |
Zhang [1 8] | 2 | 35 | Mildly impaired | Not reported | No | 4 days | Acute kidney injury, systemic toxicity | Hemodialysis, leucovorin, supportive care | Recovery |
Yu [1-] | 3 | 38 | Normal | No | No | 6 days | Grade IV myelosuppression, oral/skin ulcers,hepatotoxicity | Leucovorin,antibiotics,G-CSF | Recovery |
Refeno [ 19] | 4 | 29 | Normal | Not reported | Not reported | 3 days | Exfoliative dermatitis,severe pancytopenia | Leucovorin,G-CSF, corticosteroids | Recovery |
Jia [ 20] | 5 | 27 | Normal | Not reported | Not reported | 7 days | Vulvar edema with deep ulceration | Surgical debridement, leucovorin.antibiotics | Recovery |
Soysal [2 1] | 6 | 30 | Normal | Not reported | Not reported | 5 days | Myelosuppression, severe mucositis | Prolonged leucovorin,G-CSF.supportive care | Recovery |
lsaacs [2 2] | 7-A | 34 | Moderately impaired | Not reported | No | 4 days | Life-threatening neutropenia | Extracorporeal MTX removal,leucovorin,G-CSF | Recovery |
7-B | 36 | Moderately impaired | Not reported | No | 6 days | Life-threatening neutropenia | Extracorporeal MTX removal,leucovorin,G-CSF | Recovery | |
Lodha [2 3] | 8 | 28 | Normal | Not reported | Not reported | 5 days | Generalised rash,cytopenia | Leucovorin,supportive care | Recovery |
Gaïes [2 4] | 9 | 31 | Normal | Not reported | Not reported | 8 days | Multi-organ failure | Leucovorin,intensive supportive therapy(unsuccessful) | Death |
SAhiN [2 5] | 10 | 33 | Dialysis-dependent | Not reported | No | 3 days | Oral ulceration,extensive rash, myelosuppression | High-frequency dialysis, leucovorin,G-CSF | Recovery |
LD‑MTX | Low-Dose Methotrexate |
OAT3 | Organic Anion Transporter 3 |
G‑CSF | Granulocyte Colony-Stimulating Factor |
ANC | Absolute Neutrophil Count |
eGFR | Estimated Glomerular Filtration Rate |
β‑hCG | Beta-human Chorionic Gonadotrophin |
| [1] | Howard SC, McCormick J, Pui CH, Buddington RK, Harvey RD. Preventing and Managing Toxicities of High-Dose Methotrexate. Oncologist. 2016; 21(12): 1471-82. |
| [2] | Xiao C, Shi Q, Cheng Q, Xu J. Non-surgical management of tubal ectopic pregnancy: A systematic review and meta-analysis. Medicine (Baltimore). 2021; 100(50): e27851. |
| [3] | Practice Committee of American Society for Reproductive M. Medical treatment of ectopic pregnancy: a committee opinion. Fertil Steril. 2013; 100(3): 638-44. |
| [4] | Shaikh N, Sardar M, Raj R, Jariwala P. A Rapidly Fatal Case of Low-Dose Methotrexate Toxicity. Case Rep Med. 2018; 2018: 9056086. |
| [5] | Refeno V, Rasamimanana NG, Abasse BA, Ramarokoto MPM, Fanomezantsoa MJE, Randaoharison PG. Methotrexate-induced toxidermia and pancytopenia in a patient with ectopic pregnancy: a case report. Journal of Medical Case Reports. 2021; 15(1): 579. |
| [6] | Jiang R, Mei S, Zhao Z. Leucovorin (folinic acid) rescue for high‐dose methotrexate: A review. Journal of Clinical Pharmacy and Therapeutics. 2022; 47(9): 1452-60. |
| [7] | Chan BS, Bosco AA, Buckley NA. Navigating methotrexate toxicity: Examining the therapeutic roles of folinic acid and glucarpidase. Br J Clin Pharmacol. 2025; 91(3): 628-35. |
| [8] | Ghannoum M, Roberts DM, Goldfarb DS, Heldrup J, Anseeuw K, Galvao TF, et al. Extracorporeal Treatment for Methotrexate Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup. Clin J Am Soc Nephrol. 2022; 17(4): 602-22. |
| [9] | Deng J, Chen L, Xue H, Zeng FX, Niu PG, Shi DH. Contribution of genetic polymorphism of methylene tetrahydrofolate reductase on the effect of methotrexate in ectopic pregnancy patients. J Clin Lab Anal. 2020; 34(1): e23030. |
| [10] | Hamed KM, Dighriri IM, Baomar AF, Alharthy BT, Alenazi FE, Alali GH, et al. Overview of Methotrexate Toxicity: A Comprehensive Literature Review. Cureus. 2022; 14(9): e29518. |
| [11] | Yu H, Wang W, Liang H, Wang K, Ling B. Severe Adverse Toxic Effects of Low-Dose Methotrexate Treatment on an Ectopic Pregnancy Patient With Methylenetetrahydrofolate Reductase Mutations: A Case Report. Front Med (Lausanne). 2021; 8: 738315. |
| [12] | Wang S, Zuo S, Liu Z, Ji X, Yao Z, Wang X. Association of MTHFR and RFC1 gene polymorphisms with methotrexate efficacy and toxicity in Chinese Han patients with rheumatoid arthritis. Journal of International Medical Research. 2020; 48(2): 0300060519879588. |
| [13] | Huang J, Fan H, Qiu Q, Liu K, Lv S, Li J, et al. Are gene polymorphisms related to adverse events of methotrexate in patients with rheumatoid arthritis? A retrospective cohort study based on an updated meta-analysis. Therapeutic Advances in Chronic Disease. 2020; 11: 2040622320916026. |
| [14] | Vial T, Patat AM, Boels D, Castellan D, Villa A, Theophile H, et al. Adverse consequences of low-dose methotrexate medication errors: data from French poison control and pharmacovigilance centers. Joint Bone Spine. 2019; 86(3): 351-5. |
| [15] | Dasari P, Sagili H. Life-threatening complications following multidose methotrexate for medical management of ectopic pregnancy. Case Reports. 2012; 2012: bcr0320126023. |
| [16] | Willner N, Storch S, Tadmor T, Schiff E. Almost a tragedy: severe methotrexate toxicity in a hemodialysis patient treated for ectopic pregnancy. European journal of clinical pharmacology. 2014; 70: 261-3. |
| [17] | Isaacs Jr JD, McGehee RP, Cowan BD. Life-threatening neutropenia following methotrexate treatment of ectopic pregnancy: a report of two cases. Obstetrics & Gynecology. 1996; 88(4): 694-6. |
| [18] | Stavros S, Potiris A, Gerede A, Zikopoulos A, Giourga M, Karasmani C, et al. Methotrexate-Induced Toxicity After Ultrasound-Guided Intragestational Injection in a Patient with Caesarean Scar Pregnancy—A Case Report. Medicina. 2024; 60(11): 1900. |
| [19] | Zhang L, Liu C, Xiao L, Liu Y. Low-dose methotrexate-induced renal failure in a patient with ectopic pregnancy: a case report. J Med Case Rep. 2023; 17(1): 119. |
| [20] | Jia G, Chai W, He Z, Liu X, Wen Y, Cui L, et al. Low-dose methotrexate-induced vulvar edema: A case report. Medicine. 2019; 98(35). |
| [21] | Soysal S, Anık İlhan G, Vural M, Yıldızhan B. Severe methotrexate toxicity after treatment for ectopic pregnancy: A case report. Journal of Turkish Society of Obstetric and Gynecology. 2016; 13(4): 221-3. |
| [22] | Isaacs JD, McGehee RP, Cowan BD. Life-threatening neutropenia following methotrexate treatment of ectopic pregnancy: A report of two cases. Obstetrics & Gynecology. 1996; 88(4, Part 2): 694-6. |
| [23] | Lodha S, Mali K. Case report on toxicity of methotrexate in tubal ectopic pregnancy. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2020; 9(7). |
| [24] | Gales E, Ben Sassi M, Charfi R, Lakhal M, Klouz A, Trabelsi S, et al. Fatal methotrexate toxicity in a patient treated for an ectopic pregnancy. Therapy. 2016; 71. |
| [25] | ŞAhİN G, Acet F, Tavmergen GÖKer EN, Tavmergen E. Caution: Even in A Single-Low Dose Methotrexate for Treatment of Ectopic Pregnancy Could Have Severe Adverse Effects in Women with Chronic Renal Insufficiency: A Case Report. Türk Üreme Tıbbı ve Cerrahisi Dergisi. 2021; 5(2): 66-9. |
APA Style
Cheng, J., Xie, W., Wu, X., Li, P. (2026). Low-dose Methotrexate Toxicity in Ectopic Pregnancy: A Case Report and Literature Review. Journal of Gynecology and Obstetrics, 14(1), 30-36. https://doi.org/10.11648/j.jgo.20261401.13
ACS Style
Cheng, J.; Xie, W.; Wu, X.; Li, P. Low-dose Methotrexate Toxicity in Ectopic Pregnancy: A Case Report and Literature Review. J. Gynecol. Obstet. 2026, 14(1), 30-36. doi: 10.11648/j.jgo.20261401.13
AMA Style
Cheng J, Xie W, Wu X, Li P. Low-dose Methotrexate Toxicity in Ectopic Pregnancy: A Case Report and Literature Review. J Gynecol Obstet. 2026;14(1):30-36. doi: 10.11648/j.jgo.20261401.13
@article{10.11648/j.jgo.20261401.13,
author = {Jia-Chen Cheng and Wen-Yang Xie and Xue Wu and Pu Li},
title = {Low-dose Methotrexate Toxicity in Ectopic Pregnancy:
A Case Report and Literature Review},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {30-36},
doi = {10.11648/j.jgo.20261401.13},
url = {https://doi.org/10.11648/j.jgo.20261401.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.13},
abstract = {Low-dose methotrexate (LD‑MTX) is widely regarded as a safe and effective fertility‑preserving treatment for selected ectopic pregnancies; however, rare cases of severe, life‑threatening toxicity have been reported. We describe a previously healthy 24‑year‑old woman who developed fulminant systemic toxicity following a single intramuscular dose of 60 mg methotrexate administered for persistent tubal ectopic pregnancy after laparoscopic salpingostomy. Within 72 hours, she presented with progressive mucocutaneous manifestations, including diffuse rash, facial oedema and severe oral ulceration, followed by pancytopenia and acute kidney injury by day 4. Concomitant treatment with long‑acting benzathine penicillin G and subsequent pharmacogenetic testing revealing heterozygous MTHFR C677T and MTRR A66G variants were considered contributory risk factors. Prompt initiation of high‑dose intravenous leucovorin rescue, alkalinised hydration and granulocyte colony‑stimulating factor led to complete haematological recovery by day 14 and normalisation of renal function without the need for glucarpidase or extracorporeal clearance. A review of the literature identified fewer than a dozen similar cases, highlighting consistent early mucocutaneous warning signs and rapid progression to severe myelosuppression. This case underscores that even a single LD‑MTX dose can precipitate severe toxicity when renal clearance is impaired, interacting medications are present and folate‑pathway polymorphisms coexist, and emphasises the critical importance of early symptom recognition, close laboratory monitoring between days 4 and 7, and timely leucovorin rescue.},
year = {2026}
}
TY - JOUR T1 - Low-dose Methotrexate Toxicity in Ectopic Pregnancy: A Case Report and Literature Review AU - Jia-Chen Cheng AU - Wen-Yang Xie AU - Xue Wu AU - Pu Li Y1 - 2026/01/30 PY - 2026 N1 - https://doi.org/10.11648/j.jgo.20261401.13 DO - 10.11648/j.jgo.20261401.13 T2 - Journal of Gynecology and Obstetrics JF - Journal of Gynecology and Obstetrics JO - Journal of Gynecology and Obstetrics SP - 30 EP - 36 PB - Science Publishing Group SN - 2376-7820 UR - https://doi.org/10.11648/j.jgo.20261401.13 AB - Low-dose methotrexate (LD‑MTX) is widely regarded as a safe and effective fertility‑preserving treatment for selected ectopic pregnancies; however, rare cases of severe, life‑threatening toxicity have been reported. We describe a previously healthy 24‑year‑old woman who developed fulminant systemic toxicity following a single intramuscular dose of 60 mg methotrexate administered for persistent tubal ectopic pregnancy after laparoscopic salpingostomy. Within 72 hours, she presented with progressive mucocutaneous manifestations, including diffuse rash, facial oedema and severe oral ulceration, followed by pancytopenia and acute kidney injury by day 4. Concomitant treatment with long‑acting benzathine penicillin G and subsequent pharmacogenetic testing revealing heterozygous MTHFR C677T and MTRR A66G variants were considered contributory risk factors. Prompt initiation of high‑dose intravenous leucovorin rescue, alkalinised hydration and granulocyte colony‑stimulating factor led to complete haematological recovery by day 14 and normalisation of renal function without the need for glucarpidase or extracorporeal clearance. A review of the literature identified fewer than a dozen similar cases, highlighting consistent early mucocutaneous warning signs and rapid progression to severe myelosuppression. This case underscores that even a single LD‑MTX dose can precipitate severe toxicity when renal clearance is impaired, interacting medications are present and folate‑pathway polymorphisms coexist, and emphasises the critical importance of early symptom recognition, close laboratory monitoring between days 4 and 7, and timely leucovorin rescue. VL - 14 IS - 1 ER -
The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, China
The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, China
The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, China
The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, China